Introduction
Concussion, a form of mild traumatic brain injury, is a prevalent and complex health issue that affects the brain and leads to decline in quality of life. Commonly described as a ‘silent epidemic,’ an estimated 1.8–3.9 million sport-related concussions occur annually in the USA, while values in Canada range between 1 per 100,000 and 1% of the population per year,1–3 the majority of these injuries are sustained by youth and adolescents under the age of 18. In addition to concerns surrounding epidemiology and incidence rates, there is growing awareness of the long-term and cumulative health effects of a concussive injury, particularly in the context of a developing brain.4–6 The effects of concussion have been extensively documented, with symptoms such as somatic, mood, emotional and sleep-related disturbances being commonly reported.7,8 Concussion can further lead to deficits in cognitive and motor function, including slower processing speed,9 increased reaction time (RT),10 slower upper limb velocity and poorer accuracy.11 Previous work from our group has additionally shown declines in rule-based movement control among those with any history of concussion.12–14 Rule-based skilled performance is crucial to successful and purposeful indirect interactions with the world around us, including during sports participation. For instance, if a soccer player is attempting to pass the ball to a teammate on the right, while running to the left and simultaneously attending to other players on the field, spatial dissociations exist between vision, attention and the required motor action. In order to effectively complete this task, the player’s brain is required to combine thought and action during motor planning; this process is known as cognitive-motor integration (CMI). In contrast, daily movements that involve direct interactions with an object, or ones in which the visual stimulus is also the target of the action, are typically not affected by milder brain injury.12,15,16 Importantly, though simple or direct motor function may have recovered once individuals return to daily activity, lingering deficits in CMI ability may remain. Thus, there is a need for concussion assessments and recovery protocols to take CMI into account when considering return to play, return to work, or, more generally, return to daily life. Altogether, these behavioral disruptions may be related to functional and microstructural injuries that occur at the cellular level.17–19
Neuronal perturbations may alter brain function and contribute to observed behavioral impairments both during and after recovery, and may leave the brain more vulnerable to the effects of repetitive concussion. Findings from animal studies reveal that rodents subjected to three or more concussive insults experience greater neurodegeneration, neuroinflammation and deficits in long-term potentiation compared with those subjected to one injury.20–23 It has been suggested that repeated injuries increasingly damage the blood–brain barrier (BBB) and permit bidirectional passage of inflammatory cells, which amplifies inflammatory responses. Furthermore, larger impairments in sensory and motor functioning are observed in animals with three or more concussions compared with those with one or no concussion.22–25 Comparably, humans with a history of multiple concussions are at increased risk for re-injury,26 longer recovery,27 neurocognitive impairment,28 and neurodegenerative disease development,29 though less is known about the relationship between repetitive injury and motor control. Importantly, most of the work investigating multiple concussions in humans does not identify when deficits from previous injury may become cumulative. Nevertheless, taken together, the body of literature appears to suggest a potential threshold of three concussions, at which point blood–brain barrier breakdown and associated neuroinflammatory responses may result in long-term behavioral, sensory and motor deficits.
Several other factors are important to consider with respect to concussion recovery and the long-term effects, such as sport experience, sex and age. Previous studies have demonstrated that among asymptomatic athletes with a history of concussion, years of sport experience and skill level result in smaller CMI performance decrements, as well as a quicker recovery of this ability.16,30 Age has also been shown to be a risk factor for mild traumatic brain injury. Concussion is a common injury among children and youth, as evidenced by the fact that children have higher rates of incidence compared with adults.1 Collectively, these findings suggest that age and sport experience, and the interaction between these factors, may be especially important in determining how one may recover from mild brain injury. Finally, there is some evidence that adolescent girls and women may have greater incidence rates of concussion, express different symptoms and experience longer recovery times.31–33 These sex-related differences may be related to hormonal influences, differences between males and females in neck musculature and strength, and cerebral blood flow and metabolic differences.34–36 Thus, the purpose of the current study was to examine the effects of age, sport experience and multiple concussion history on performance in simple eye–hand coordination and multidomain CMI tasks. We hypothesized that relative to those with one concussion, those with multiple concussions would experience significantly greater neuropathological effects on the brain networks required for standard and rule-based visuomotor performance. Therefore, we predicted that variance in CMI performance, which is reflective of brain network function, would be explained by number of previous concussions (one vs. more than one), after accounting for age and athletic experience. A secondary, exploratory aspect of our study was to investigate the effect of sex in this performance.
Materials & methods
Participants
Two hundred twenty-three asymptomatic individuals (18.9 ± 7.0 years, range: 9–53 years; 29.2% female) with a history of 1– 10 concussions (mean number of concussions 1.7 ± 1.4) and varying levels of sport experience participated in this study. Participants were separated into four age groups (9–13, 14–19, 20–25, 26 years old and older), since cognitive-spatial and motor abilities have been shown to be affected by developmental age and brain development.7,8,37–41 Specifically, cognitive and motor performance differs between the ages of 9 and 13, 13 and 16, 19 and 22, and 20 and 25, and this performance is related to BOLD activity.8,38,39 Similarly, total brain volume, as well as grey and white matter, peaks and continues to develop through the teenage years and into the early twenties.36,37 Thus, in attempt to account for these developmental windows, we grouped our data by logically relevant timeframes. Moreover, we obtained information about concussion history and demographic data from our own and established questionnaires (SCAT3/5, Child-SCAT3/5), and for select/elite athletes, through interviews with participants, their parents, team managers and coaches. The concussion history assessment was based on self-report. However, participants were only included in the study if they reported that concussions were medically diagnosed. With respect to concussion number, estimated incidence rates suggest that a majority of youth in this age range have experienced one concussion versus more than one, an estimate that is reflected in our sample having 68% individuals with one concussion.42 For this reason as well as reasons of statistical power, participants were grouped into one concussion or more than one concussion. All participants in this study were athletes who played sports at varying levels. Therefore, sport experience was determined based on the level of sport engagement: recreational athletes, select athletes who played competitively and elite level athletes. Athletes who played at higher levels of competition were thus considered to have had more sport experience as greater levels of commitment, training and competition are required. Table 1 summarizes the participant demographics. At the time of testing, all participants were reported to be healthy, not diagnosed with a current concussion, and if applicable, were fully participating in their team sport. All participants were recruited from the community. Testing took place in the local community between 2012 and 2018. The study protocol was approved by York University’s Ethics Review Board (the Human Participants Review Committee) and conformed to the standards of the granting agency’s Research Ethics guidelines. Participants, parents and coaches signed written informed consent/assent forms before participating in this study.
Procedures
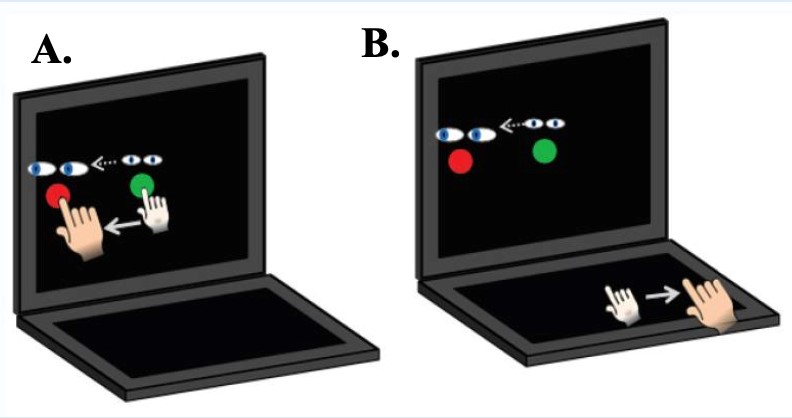
Participants performed two visuomotor transformation tasks that required sliding the index finger of their dominant hand from a central target towards a peripheral target (top, left, right or bottom) on an Acer Iconia 6120 dual-touch screen tablet, which has touchscreens in the vertical and horizontal plane, or on an ASUS touchscreen tablet (Asus Transformer Book T100TAF) with an externally connected USB touchpad (Keytec™, TycoTouch, USA) situated perpendicular (in the horizontal plane) to the ASUS screen. In the standard (direct) condition, the spatial location of the viewed target and the required movement were in alignment (hand movements were made directly to the peripheral targets (Figure 1A). The CMI condition was a nonstandard visuomotor task that included two levels of decoupling: participants viewed the targets on the vertical touchscreen, but had to slide their finger along the horizontal screen and in the opposite direction to the presented target in order to displace the cursor (feedback reversal). For example, moving the cursor left required participants to slide their finger right (Figure 1B). The order of conditions was randomized in order to control for potential learning effects.
**_standard_motor_task_condition__location_of_eye_and_hand_targets_are_in_spatial_ali.jpg)
For each trial, a yellow home target was presented in the center of the screen; once participants guided the cursor toward its center, this target became green. After a delay period of 2000 ms, a red peripheral target was then presented to the top, bottom, right or left of the center target, serving as a ‘go’ signal for the participant to look at and slide towards this target. Once the peripheral target was held for 500 ms, it disappeared, signaling the end of the trial. The next trial began with the reappearance of the central target following an inter-trial interval of 2000 ms. Each participant completed 20 trials per condition (five trials to each peripheral target), with peripheral targets presented in a random order. In both conditions, participants were instructed to move as quickly and as accurately as possible.
Data processing & analysis
Kinematic measures, including timing, finger position and error data were recorded for each trial and converted into a binary readable format using a custom written C++ application. Trials were deemed errors if the finger left the home target too early (<2000 ms), reaction time (RT) was too short (<150 ms), RT was too long (>8000 ms) or movement time was too long (>10,000 ms). Trials in which the first ballistic movement exited the boundaries of the center target in the wrong direction (greater than 45° from a straight line to the target) were coded as direction reversal errors and were analyzed as a separate variable. A custom-written analysis program (using Matlab, Mathworks, Inc., USA) was used to generate a computerized velocity profile of each trial’s movement, with movement onset and end being recorded at 10% peak velocity. These profiles were then verified by visual inspections and corrections were performed when necessary. The scored data were processed to compute six different movement timing and execution outcome measures.
Dependent visuomotor performance measures
The dependent variables of interest were reaction time (RT), movement time, path length, peak velocity, accuracy, precision and the percent of trials that involved a movement direction reversal after the movement had begun. These kinematic variables were categorized as either timing variables or path variables.
Movement timing variables
RT was calculated as the time interval (milliseconds; ms) between the disappearance of the central target and movement onset. Full movement time (fMT) was calculated as the time in ms between movement onset and offset. Peak velocity (PV) was the maximum velocity in mm/ms during the ballistic movement obtained for each trial.
Movement path variables
Full pathlength (fPL) was calculated as the distance between the start and final end location of the cursor movement. Thus, movements including curves or deviations from a straight-line path between the central and peripheral target would result in a longer pathlength. Absolute error (AE), the endpoint accuracy, was calculated as the distance between the mean individual movement end points and the actual target location (defined as its center), in mm. Variable error, the end point precision was determined as the distance between the end points of individual movements (σ2) from their mean movements, measured in mm.
Statistical analysis
Relationship between performance and participant characteristics
The primary aim of this analysis was to investigate the amount of variability in visuomotor performance that could be predicted by our variables of interest. Thus, multiple linear regression analyses were used to assess if previous number of concussions (one vs. multiple concussions), athletic experience (recreational, select, professional-level), age (9–13, 14–19, 20–25 and 26 years old and up) and sex (male vs. female) could significantly predict the variability of the six dependent kinematic variables in both the standard and CMI conditions. Forward stepwise regression was used to select the best regression models in accounting for performance variance for each dependent variable (n = 6), in both conditions (n = 2), and independent variables that were statistically significant were included in the models.
Trials containing outcome measures >2 standard deviations away from the mean for a given condition in a given participant were considered outliers and removed before statistical analysis. All remaining data were checked for normal distribution and sphericity (Mauchly’s test), and were Greenhouse–Geisser corrected where necessary. Statistical analyses were performed using SPSS statistical software (IBM Inc.). Statistical significance levels were set to α ≤ 0.05.
Results
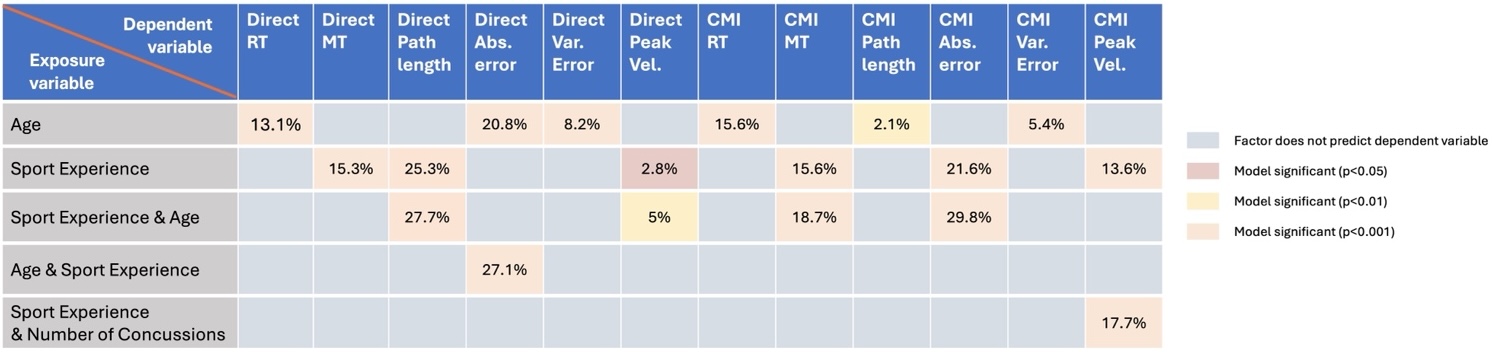
Linear regression of the factors associated with basic and complex visuomotor performance are presented in Table 2. Of the four factors (number of concussions, sex, age and sport experience), age, sport experience and number of concussions were found to significantly predict variability in movement performance.
Movement timing variables
We observed that age (13 years old and under, 14–19, 20–25, 26 and older) was the only factor that could predict variability in RT for basic and complex rule-based visuomotor performance (standard task: R2 = 0.131, F(1, 214) = 32.279, p < 0.001); CMI task: R2 = 0.156, F(1, 213) = 39.475, p < 0.001). In addition, sport experience significantly explained 15.3% of the variance in fMT in the standard condition (R2 = 0.153, F(1, 213) = 38.535, p < 0.001). In the CMI condition, sport experience was entered in the first step and was found to significantly explain variance in visuomotor performance (R2 = 0.156, F(1, 213) = 39.400, p < 0.001). However, the final model, which included both sport experience and age, demonstrated a stronger fit and thus accounted for a greater proportion of variability in fMT (R2 = 0.187, F(2, 212) = 24.392, p < 0.001). Finally, both sport experience and age were significantly associated with variability in PV during standard and CMI performance. In the standard condition, a small amount of variance was explained by sport experience (R2 = 0.028, F(1,196) = 5.560, p = 0.019), although including age in the model modestly strengthened the fit (R2 = 0.050, F (2,195) = 5.107, p = 0.007). In contrast, 13.6% of the variance of PV in the CMI condition was explained by sport experience (R2 = 0.136, F (1,199) = 31.340, p < 0.001) and an additional 4% of PV variability was explained by adding the number of concussions to the model (R2 = 0.177, F (2,198) = 21.335, p < 0.001).
Movement execution variables
We observed that sport experience significantly explained 25% of the variance in fPL in the standard condition (R2 = 0.253, F (1, 213) = 72.045, p < 0.001); this was moderately improved by the inclusion of age in the model (R2 = 0.277, F (2, 212) = 40.675, p < 0.001). In contrast, age alone was associated with small amounts of variability in performance in the CMI condition (R2 = 0.021, F (1, 213) = 4.641, p = 0.032). Furthermore, variability in AE was significantly predicted by sport experience and age. Specifically, 23% of the variance in AE was explained by age in the standard condition (R2 = 0.208, F (1, 214) = 56.372, p < 0.001), and a further 7% of this variance was predicted by including sport experience in the model (R2 = 0.271, F (2, 213) = 39.586, p < 0.001). Finally, age was the only factor significantly associated with variable error in the standard (R2 = 0.082, F(1,192) = 17.243, p < 0.001) and CMI conditions (R2 = 0.054, F(1,196) = 11.284, p < 0.001).
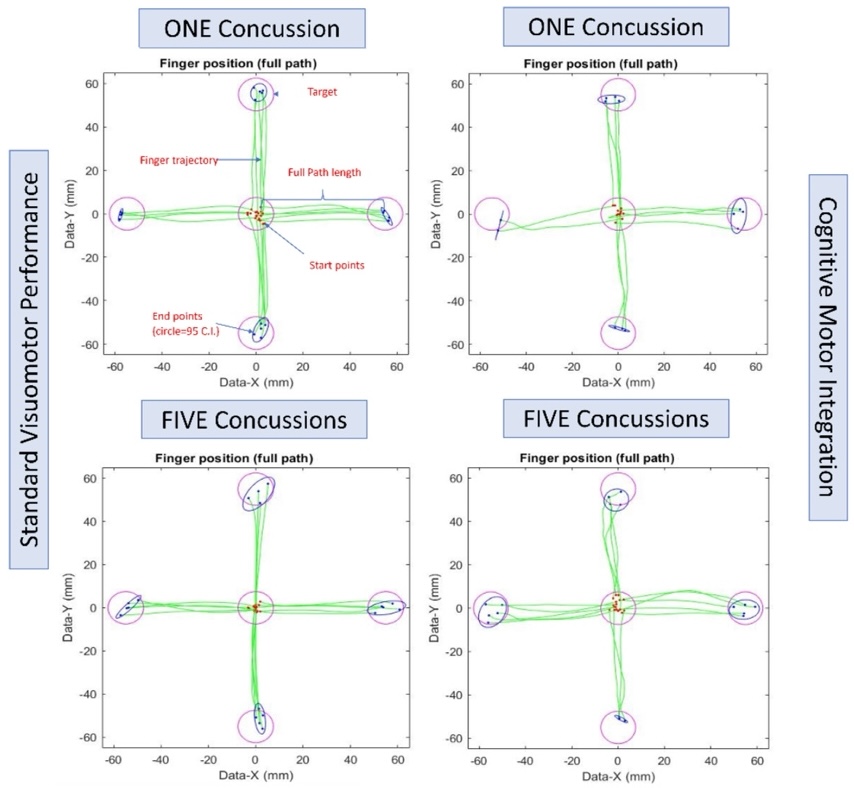
In summary, the results from these multiple regression analyses emphasize the importance of sport experience and age in explaining visuomotor ability. Notable is the fact that except for PV, the number of concussions was not a significant predictor of variance for our movement performance measures (Figure 2). Figure 3 presents a set of typical movement trajectories for both the standard and CMI tasks demonstrating performance differences observed in this study. Note that the basic visuomotor skill is somewhat affected by number of concussions (top vs. bottom left, see greater end point variability), but CMI visuomotor behavior is not obviously much worse as a function of concussion number (top right vs. bottom right).


Discussion
This study sought to determine the extent to which the variability in standard and CMI task performance could be explained by previous number of concussions, sex, age and sport experience among asymptomatic individuals with a history of concussion. Contrary to our hypothesis, we did not find that the number of concussions accounted substantially for differences in skilled visuomotor performance. Rather, we observed that in our sample comprised mostly of younger and mainly select-level athletes, a significant percentage of variance was primarily explained by age and sport experience. In particular, accounting for these variables was essential in order to meaningfully predict skilled visuomotor performance among individuals with any number of concussions. Finally, no sex-related differences were observed in this population.
The results of the current study suggest that the damaging effects of repetitive brain injury may be related to the level of sport experience when engaging in a rule-based movement task. The planning and execution of standard and rule-based complex tasks requiring CMI relies on the integrity of parietofrontal networks, as well as on communication between cortical and subcortical movement control regions.43,44 Based on work examining CMI networks in human and nonhuman primates,43–47 we have previously suggested that disruptions within these networks, whether due to impairments in communication, microstructural injury, or both, may underlie deficits in complex visuomotor task performance following concussion.12,14 Here, we observe that in a broad demographic sample, sport experience can explain variability in standard and CMI task performance. Thus, these findings suggest that skilled experience may provide resilience to injury in motor control brain networks, and this may compensate for concussion-related performance declines. This idea is consistent with the results from previous concussion history studies among athletes, in which an inverse relationship between CMI deficits and skill level was found.13,48 Indeed, multiple studies have shown greater neural efficiency among various types of elite performers, as evidenced by reduced cortical activation.48–50 It has been posited that this is reflective of differences in the level of effort required to produce movement between novice and skilled performers.48,49 Specifically, it is suggested that expert and elite athletes (and performers more generally, such as musicians and video gamers) require less neuronal recruitment and thus minimal energy consumption when engaging in skilled motor action. In contrast, novice performers require increased and highly controlled motor planning, and experience lower levels of automaticity.51,52 In individuals with more sport experience, these superior networks may consequently lessen the impact of neurophysiological changes associated with concussion and may thus lead to enhanced performance. Similar to ‘cognitive reserve’, this ‘motor reserve’ may serve as a protective effect against further injury upon return to activity. Of note, however, is that all participants in this study were active in sport to some level. Thus, it remains to be shown whether this capacity for motor reserve will continue to be observed when children, adolescents and young adults with skilled experience (e.g., sport or music) are compared with more sedentary individuals, and how they will respond in terms of recovery. Or, rather, whether this observation is due to the higher performance of athletes at baseline compared with a broader population. Thus, a future study will compare how motor performance differs following multiple concussion history in skilled and unskilled youth and young adults.
We additionally found a significant effect of age in explaining movement performance variance. This observation supports the notion that motor developmental stages may compensate for the pathophysiological effects of concussion, and may thus contribute to motor control reserve. It is well established that developmental age affects motor ability in general, with more basic motor functions, such as goal-directed reaching or grasping, emerging earlier in childhood than more skilled ones, which may not peak until late childhood or adolescence.53,54 In particular, the ability to integrate rule-based elements of cognition into a required motor action (i.e., the ability to successfully execute movements requiring CMI) has been shown to mature in late childhood.10 Accordingly, if a concussion is sustained, a younger, developing brain may be more neurologically fragile for executing complex behaviors, since these functions may not have fully matured at the time of injury. The rate at which these abilities develop can therefore help explain why young athletes are more vulnerable to the effects of concussion compared with adolescents or adults.41,55,56 In the context of sport, the ability to concurrently integrate aspects of cognition and complex motor function is vital to successful performance. In fact, among children and adolescents with a concussion history, impairments in movement timing and execution have been demonstrated.14,57 Concussed youth have been further shown to have slower gait patterns during cognitive-motor dual-tasks58 and take longer to complete tasks requiring fine motor skills.59 These impairments are exhibited past the recovery period. Overall, these findings, in combination with results from the present study, may reflect that developmental age, and the associated stage of motor development, may lead to stronger networks controlling the performance of complex, rule-based movements, and this may dampen the deleterious impacts of previous injury in individuals with multiple concussion history.
Performance in motor tasks assessing RT and speed has been shown to differ between males and females,60,61 and sex-related differences have been observed more generally in tasks requiring eye–hand coordination.62,63 However, no effects of sex were observed in this study. The lack of sex-related differences may be related to the fact that, contrary to previous work investigating sex differences in motor control, many of our participants were younger and pre/peri-pubescent. Thus, potential sex differences due to hormonal influences may not have been evident in this sample. Nonetheless, the relationships between visuomotor ability, sex and multiple brain injury require further examination in both youth and adults.
While a strength of the present study is the size of the sample of individuals with concussion history who also performed a well-controlled visuomotor task, a limitation is in the range of values within each of the factors that we examined. Future work will expand on findings from the present study by examining the effects of multiple concussion (three or more), age, sex and sport experience in a broader and larger sample. Our findings suggest that motor network resiliency may underlie the greater weighting of sport experience and developmental age in this younger sample, over multiple concussion history and sex. An important open question is at what age after full development will this resiliency no longer compensate for the long-term neural effects of repeated head impacts, given age-related psychomotor slowing60 and hormonal changes. Our ongoing research examines these factors in working-aged and older adults, as well as in retired athletes. This may allow us to answer important remaining questions, including when neural movement control resiliency may become less effective, how many concussions may be ‘too many,’ and which factor – sport experience or age – plays a more important role in complex skilled performance. Concussion history, and specifically multiple concussion history, are risk factors for cognitive impairment, challenges with mental health, motor dysfunction and neurodegenerative conditions. Therefore, developing an improved understanding of the effects of various factors that impact one’s movement control response to mild brain injury may allow for targeted approaches that aim to strengthen the brain networks affected by concussion. Accounting for such factors may ultimately result in the preservation of functional abilities despite injury.
Conclusion
The results of the present study emphasize the clinical importance of accounting for sport experience and age when assessing the effects of multiple concussion on complex visuomotor skill. Most return to sport, school and work assessments do not include multidomain integration tasks such as CMI, and often do not take demographic factors into account during recovery. Therefore, these assessments may not fully capture functional ability following brain injury and may thus result in a premature return to full daily life activities. We suggest that taking into account individual differences, in addition to examining performance that requires the integration of cognition and action, is a useful and important approach in order to comprehensively assess brain function following concussion.
Conflict of Interest
The authors have no conflicts of interest to declare.
Financial disclosure
Canadian Institutes of Health Research #MOP-125915; Natural Sciences and Engineering Research Council of Canada #2016-05336; Canada First Excellence Fund Vista Research Chair.
Ethical conduct of research
The study protocol was approved by York University’s Ethics Review Board (the Human Participants Review Committee) and conformed to the standards of the granting agency’s Research Ethics guidelines. Participants, parents and coaches signed written informed consent/assent forms before participating in this study.